%20(4%20x%206%20in)_20260116_175012_0000.jpg)
Get care
At Northwest Referrals, we understand how concerning a diagnosis of hip dysplasia can be for pet owners.
Our advanced team is dedicated to providing advanced diagnostics, tailored treatment plans, and compassionate care to help your dog stay active, comfortable, and happy for as long as possible.






During the first weeks of life, the soft tissue structures responsible for joint stability, including the joint capsule and supporting ligaments, become progressively lax. This laxity disrupts the normal congruency of the hip joint, which functions as a ball-and-socket articulation. As instability persists, the femoral head becomes flattened and deformed, while the acetabulum becomes shallower and more saucer-shaped.
All dogs affected by hip dysplasia will develop secondary osteoarthritis in the involved joints. In the majority of cases, the condition affects both hips (bilateral involvement).

This condition is primarily genetic in origin, with current evidence suggesting that it is influenced by the interaction of more than one hundred genes. However, environmental factors may play a role in determining whether a genetically predisposed individual goes on to develop clinically significant disease.
For example, factors such as obesity during growth can exacerbate the expression of the condition. It is important to emphasise that environmental influences do not cause hip dysplasia; rather, they may affect the severity or clinical manifestation in dogs that are already genetically predisposed.
There is no scientific evidence to support the notion that excessive exercise during puppyhood contributes to the development of hip dysplasia.
Hip dysplasia is the most common orthopaedic disorder in dogs. It is seen most frequently in large, rapidly growing breeds, although smaller dogs and cats may also be affected.
The onset of clinical signs is variable, but the condition is most commonly diagnosed between 6 and 12 months of age. Clinical presentation can vary widely and may include stiffness, reduced exercise tolerance, difficulty rising or lying down, reluctance or difficulty in climbing stairs, and gait abnormalities such as lameness affecting one or both pelvic limbs.
Overt signs of pain are often subtle or absent in the home environment. However, affected dogs frequently exhibit significant discomfort during clinical examination, particularly when the hips are extended by a veterinary surgeon.
Pain initially arises from repetitive strain affecting the soft tissue structures that stabilise the lax hip joint, together with microfractures of the articular cartilage and subchondral bone surfaces subjected to abnormal loading and friction.
As the disease progresses and cartilage degradation advances, pain becomes primarily associated with the development of osteoarthritis, reflecting a chronic, global degenerative process within the joint.
In the first instance you may have noticed your dog exhibiting some or all of the following clinical signs;
Stiffness
Exercise intolerance
Difficulty rising, sitting or lying
Difficulty climbing stairs or getting in and out of the car
Abnormal gait – ‘swaying’ gait during walk
Limping on one or both hind limbs
Protective of hip region during grooming or bathing
Pain
Your primary care veterinary surgeon may identify abnormalities in your dog’s gait or detect discomfort in the hips during a routine examination or following concerns you have raised. If hip dysplasia is suspected, radiographic evaluation of the hip joints may be performed. In many cases, radiographs will demonstrate characteristic changes, although early or mild cases may not always be clearly evident. Dogs with suspected hip dysplasia are commonly referred for further assessment by an orthopaedic surgeon.
Following referral to the orthopaedic service at Northwest Referrals, your dog will undergo a consultation with one of the orthopaedic clinicians. This will include a comprehensive orthopaedic examination, during which a provisional diagnosis can be established and appropriate management options discussed.
Depending on the agreed diagnostic plan, your dog may be admitted for further imaging. Radiographs of the hip joints are typically obtained under sedation or general anaesthesia to ensure optimal positioning and diagnostic quality. In some cases, additional advanced imaging, such as computed tomography (CT), may be recommended and performed by the advanced diagnostic imaging team.
Throughout the process, your dog will receive dedicated one-to-one care from a member of the nursing team, all of whom are highly trained and experienced in patient preparation, sedation, and anaesthesia.

Surgical management options for hip dysplasia can be broadly categorised into procedures that aim to modify or preserve hip joint anatomy, and those regarded as salvage procedures.For further details on these techniques, please refer to the dedicated information pages for each procedure.

The optimal management of hip dysplasia is influenced by multiple factors, with the severity of clinical signs being the most significant. In some cases, dogs may exhibit only mild clinical signs, and the condition may be identified incidentally during screening examinations, for example as part of breeding assessments.
In contrast, other dogs present with more pronounced clinical signs. In these patients, treatment strategies are aimed not only at addressing the current clinical condition but also at mitigating the risk of progression and managing potential long-term complications associated with the disease.
Non-surgical management is typically recommended for dogs in which hip dysplasia is identified incidentally and is not associated with significant clinical signs. In clinically affected dogs, the success of conservative management largely depends on the severity of hip pain.
The key components of non-surgical treatment include body weight management, physiotherapy, controlled and modified exercise, and the use of medications such as non-steroidal anti-inflammatory drugs (NSAIDs). In the short term, many dogs show clinical improvement when appropriately managed. However, these improvements are often not sustained long term. A large proportion of dogs will require ongoing exercise restriction and long-term medical management, and the majority demonstrate pain on clinical examination later in life.
We work closely with local rehabilitation centres. They will perform a detailed clinical assessment and develop an individualised rehabilitation plan tailored to your dog

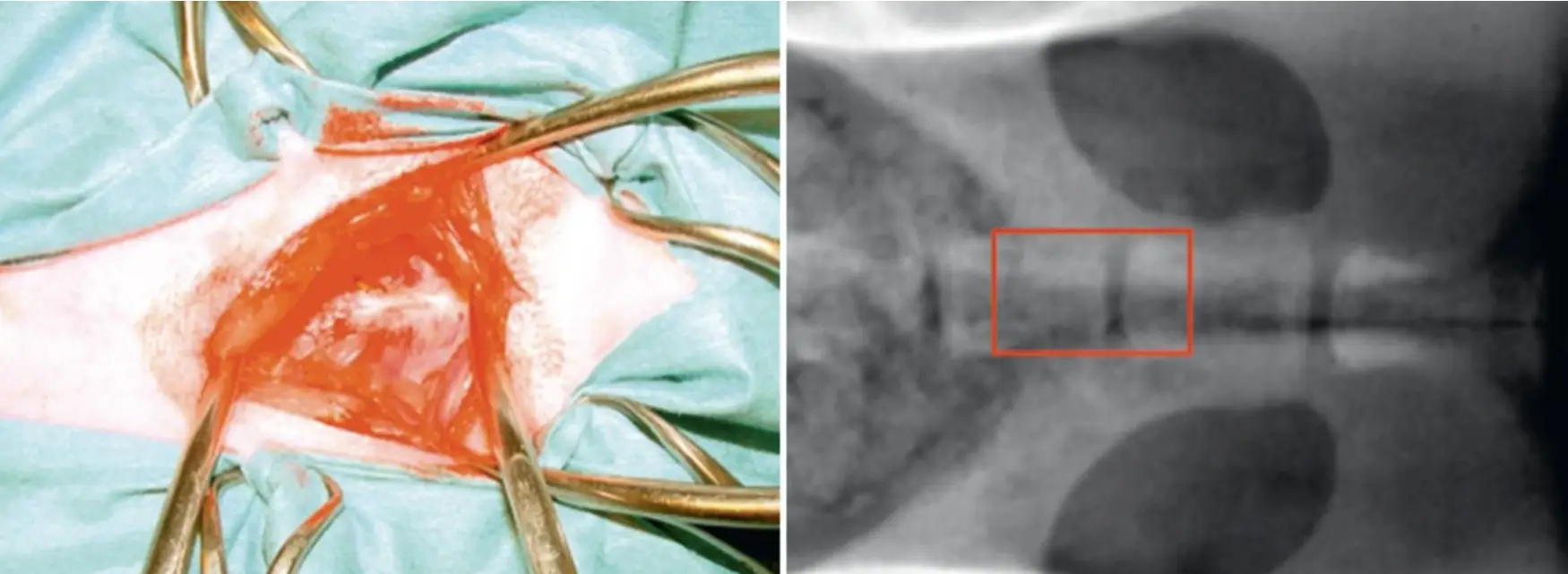
This procedure involves the induction of premature closure of a portion of the pelvis in order to influence subsequent growth and improve the positioning of the femoral head within the acetabulum.
The technique is relatively straightforward and consists of electrocauterisation of the pubic symphysis on the ventral aspect of the pelvis. For the procedure to be effective, dogs must be no older than five months of age and must demonstrate mild to moderate hip laxity, confirmed through both clinical manipulation and radiographic assessment.
As clinical signs of hip dysplasia typically do not develop until after six months of age, this procedure is generally performed as a prophylactic intervention. Dogs undergoing this treatment are routinely neutered at the same time.
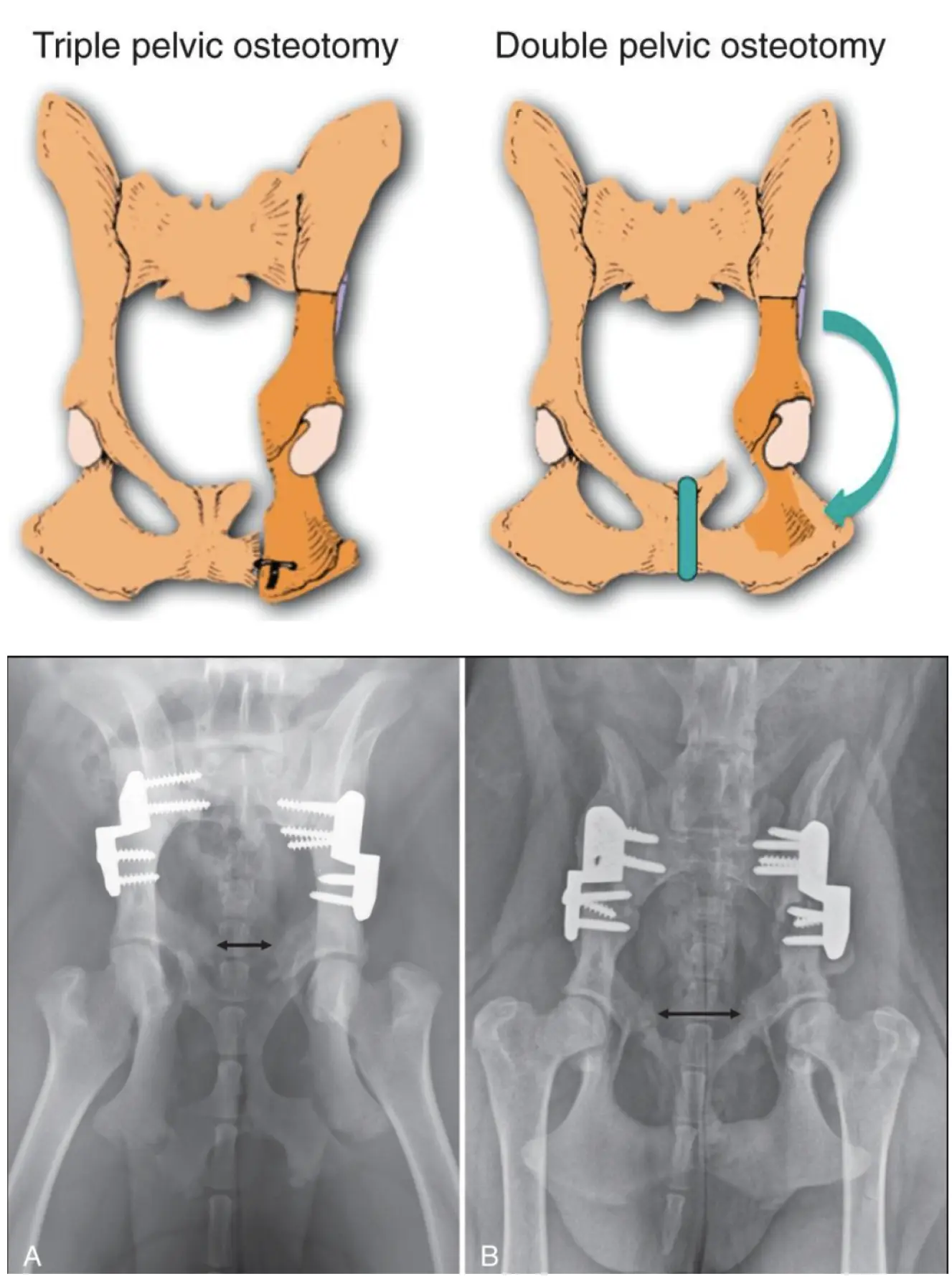
This procedure involves surgical modification of the pelvis to improve coverage of the femoral head by the acetabulum, thereby enhancing hip joint stability.
In a double pelvic osteotomy (DPO), two controlled osteotomies are performed in the pelvic bones, allowing the acetabular segment to be rotated into a position that provides improved containment of the femoral head. The repositioned bone segment is then stabilised using a specialised plate and screws designed for this procedure. Osseous healing typically occurs over a period of approximately 4–6 weeks.
DPO is indicated in dogs with hip laxity but without evidence of secondary bony remodelling or established osteoarthritis. Careful case selection is essential and involves a combination of orthopaedic examination, specific manipulative tests, and diagnostic imaging, including radiography. These assessments are carried out by experienced orthopaedic surgeons and advanced diagnostic imaging practitioners.
Suitable candidates are generally young, skeletally immature dogs. In many cases, arthroscopic evaluation of the hip joint is recommended prior to surgery to assess the integrity of the articular cartilage and confirm suitability for the procedure.
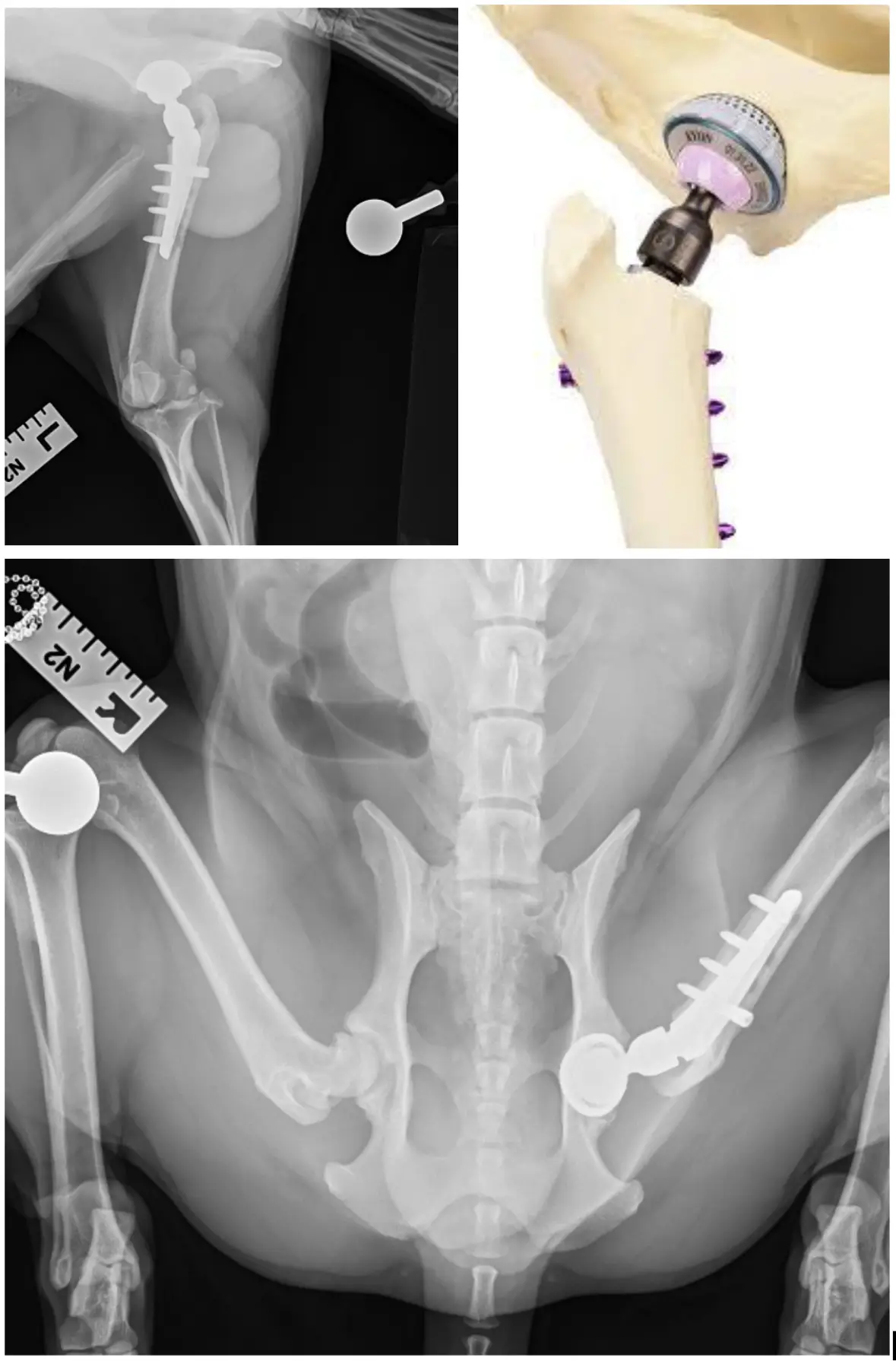
Total hip replacement (THR) is an advanced surgical procedure and should be performed only by experienced orthopaedic surgeons. It involves complete excision of the diseased hip joint, with replacement of both components of the articulation. The femoral head (“ball”) is substituted with a metal implant, while the acetabulum (“socket”) is replaced with a prosthetic component typically composed of a combination of metal and polyethylene.
Implants are secured using screws which lock into the stem.
Although THR is most commonly performed in medium to large breed dogs, it can also be successfully undertaken in smaller dogs and, in selected cases, in cats, particularly where alternative surgical options have been unsuccessful. In patients requiring bilateral intervention, procedures are staged rather than performed simultaneously to reduce the risk of complications.
Reported success rates for THR are approximately 90–95%. Most dogs show marked improvement in comfort within a few days following surgery, and many return to a high level of function and activity.
This procedure is considered a salvage option and is typically reserved for cases in which total hip replacement (THR) is not feasible, for example due to financial constraints or patient-specific anatomical factors that preclude prosthetic implantation.
The technique, commonly referred to as femoral head and neck excision (FHNE), involves complete removal of the femoral head and neck, thereby eliminating the “ball” component of the hip joint. This prevents direct bone-on-bone contact between the femur and the acetabulum, resulting in pain relief. Over time, a fibrous pseudoarthrosis (“false joint”) forms.
Although this procedure can provide satisfactory pain control, the functional outcome is variable and often less predictable than with THR, particularly in larger or more active dogs, where limb function may remain suboptimal.
Postoperative rehabilitation is essential to optimise clinical outcome.

Hear from veterinary professionals and pet owners who rely on our team for seamless referrals, clear updates, and advanced care.
I am so grateful to Northwest Referrals for operating on my dog who had IVDD of the neck for 10 weeks and was in a lot of pain.
We have been seen the next day, CT scan confirmed slipped disc already suspected after quick examination. Surgery was the same day, he has been recovering amazingly quick and well, his cut healed perfectly and we cannot thank all the team enough!
I honestly cannot rate this referral centre highly enough!
Had an MRI for my chihuahua. Results came back quickly. The vet was professional, and all the staff was very nice to us. The price was reasonable as well.
It’s always going to be expensive when it comes to being referred by your own vet. The great thing about Northwest Referrals is the costs are all up front.
If I could give 20 stars I would. I spoke to Amanda who was super helpful and gathered as much info as she could after speaking to the vets/surgeons.
We travelled from Birmingham… The bill was exactly what we had been quoted.
Not only were they a third cheaper, our assigned vet was professional and explained everything in detail.
We've streamlined our referral process to make advanced care accessible and efficient for your practice.

Your pet is seen by a named advanced practitioner who reviews their history and carries out a thorough clinical examination. We’ll discuss what we’ve found and what we recommend, in plain English.

Before any procedure begins, we provide a written, itemised estimate covering all costs: the procedure, anaesthetic, imaging, and follow-up. You’ll see exactly what you’re approving.

Once you confirm, the price is locked. We don’t add to it. If unforeseen clinical complications arise during a procedure, we discuss this with you before proceeding, we never present a surprise bill after the fact.

The prices below reflect the full cost of advanced-level diagnostics and treatment at our Wigan facility. Prices are shown all-inclusive of everything so what you see is what you get. No surprises. If you have any questions, please don't hesitate to get in touch.
Click to toggle
£1,195
Includes sedation or GA, contrast, and report from European Diplomat in Diagnostic Imaging
£1,500
Includes sedation or GA, contrast, and report from European Diplomat in Diagnostic Imaging
£2,000
Includes sedation or GA, contrast, and report from European Diplomat in Diagnostic Imaging
Imaging
Click to toggle
This includes all consumables, catheterisation, general anaesthetic, hospitalisation for one night (further days are charged at £250/night).
Plus, a post operative CT scan
£3,995
Neurology
Click to toggle
This includes pre-operative x-rays, all consumables, general anaesthetic and hospitalisation for one night.
Bilateral TPLO
£4,800
£2,500
Orthopaedics
Click to toggle
This includes all consumables, general anaesthetic and hospitalisation for one night. If bilateral it is an extra £800.
£2,000
Soft Tissue
Click to toggle
This includes all consumables, general anaesthetic and hospitalisation for one night.
With CT Scan
£3,000
£1,995
Soft Tissue
Click to toggle
This includes all consumables, general anaesthetic and hospitalisation for one night.
£1,995
Soft Tissue
Click to toggle
This includes all consumables, general anaesthetic and hospitalisation for one night.
£2,000
Soft Tissue
Click to toggle
This includes all consumables, general anaesthetic and hospitalisation for one night.
£1,295
Soft Tissue
Click to toggle
This includes all consumables, general anaesthetic and hospitalisation for one night.
£1,800
Soft Tissue
Click to toggle
This includes all consumables, general anaesthetic and hospitalisation for one night.
£1,000
Soft Tissue
Click to toggle
This includes all consumables, general anaesthetic and hospitalisation for one night.
£2,500
Soft Tissue
Click to toggle
This includes all consumables, general anaesthetic and hospitalisation for one night.
£2,000
Soft Tissue
Click to toggle
This includes all consumables, general anaesthetic and hospitalisation for one night.
£1,800
Soft Tissue
Click to toggle
This includes all consumables, general anaesthetic and hospitalisation for one night.
£2,000
Soft Tissue
Click to toggle
This includes all consumables, general anaesthetic and hospitalisation for one night.
£3,000
Soft Tissue
Click to toggle
This includes all consumables, general anaesthetic and hospitalisation for one night.
£2,500
Soft Tissue
Click to toggle
This includes all consumables, general anaesthetic and hospitalisation for one night.
£2,500
Soft Tissue
Click to toggle
This includes all consumables, general anaesthetic and hospitalisation for one night.
£800
Soft Tissue
Click to toggle
This includes all consumables, general anaesthetic and hospitalisation for one night.
£500
Soft Tissue
Click to toggle
This includes all consumables, general anaesthetic and hospitalisation for one night.
£2,500
Soft Tissue
Click to toggle
This includes all consumables, general anaesthetic and hospitalisation for one night.
£2,000
Soft Tissue
Click to toggle
£1,495
Includes sedation or GA, contrast, and report from European Diplomat in Diagnostic Imaging
£1,895
For both brain or spine, this includes general anaesthetic.
Imaging
Click to toggle
This includes all consumables, catheterisation, general anaesthetic, hospitalisation for one night (further days are charged at £250/night).
Plus, a post operative CT scan
£3,995
Neurology
Click to toggle
This includes all consumables, catheterisation, general anaesthetic, hospitalisation for one night (further days are charged at £250/night).
Plus, a post operative CT scan
£4,500
Neurology
Click to toggle
This includes all consumables, catheterisation, general anaesthetic, hospitalisation for one night (further days are charged at £250/night).
Plus, a post operative CT scan
£4,500
Neurology
Click to toggle
This includes all consumables, catheterisation, general anaesthetic, hospitalisation for one night (further days are charged at £250/night).
Plus, a post operative CT scan
£4,500
Neurology
Click to toggle
(Double plate, Y fracture and angular limb deformity) This includes pre-operative x-rays, all consumables, general anaesthetic and hospitalisation for one night.
£3,000
Orthopaedics
Click to toggle
This includes pre-operative x-rays, all consumables, general anaesthetic and hospitalisation for one night.
With a CT Scan
£3,000
£2,000
Orthopaedics
Click to toggle
This includes pre-operative x-rays, all consumables, all implants, general anaesthetic and hospitalisation for one night.
£5,800
Orthopaedics
Click to toggle
(Pin, Wire, Plate and single plate) This includes pre-operative x-rays, all consumables, general anaesthetic and hospitalisation for one night.
£2,500
Orthopaedics
Click to toggle
Cost
£4,000
Orthopaedics
Click to toggle
Cost
£3,800
Orthopaedics
Click to toggle
Cost
£2,000
Orthopaedics
Click to toggle
This includes all consumables, general anaesthetic and hospitalisation for one night. If Bilateral it is an extra £800.
£1,200
Orthopaedics
Click to toggle
£500
This includes sedation if needed and interpretation from a RCVS practitioner or a RCVS advanced practitioner in Cardiology
£500
This includes sedation if needed and interpretation from a RCVS practitioner or a RCVS advanced practitioner in Cardiology
£1,000
Full cardio work-up including x-rays, echocardiogram and consultation
Add-on CT Scan: £1,000
Imaging
Click to toggle
This includes all sedation (or general anaesthetic), as many views as needed.Including an interpretation from one of our 4 RCVS advanced practitioners
£595
Imaging
Click to toggle
Cost
Case dependent
Neurology
Whether you're a veterinary professional seeking support or a pet owner looking for advanced care, we have a clear pathway for you.
Fast online referral, 24-hour response, detailed reports, and a dedicated WhatsApp line for case queries. Your client is in the hands of an advanced practitioner from day one.
Submit a referral →
You can come directly to us, no GP-style referral required. Get a fixed-price consultation with a named advanced practitioner, with full support throughout your pet’s care.
Book a consultation →
.jpg)

%20Shepherd%20-%20CertAVP%20PgCert%20VPS%20MRCVS.jpeg)

.jpg)
%20GPCert%20Pgc(SAS)%20MRCVS%20(1).jpg)

