
Pelvic Fractures
Pelvic fractures are common, representing 20-30% of fractures in small animals. They are most commonly seen in young, healthy dogs and cats subsequent to being hit by car. Concurrent injuries to vital organs are very common, and should be addressed before definitive fracture management.
Presentation and Physical Examination
Patients with pelvic fractures may present with a mild to non weightbearing lameness. They typically present with a trauma history and almost always have a second injury, whether orthopedic or soft tissue. While pelvic fractures are painful and can result in significant blood loss, their stabilization comes second to treatment of immediately life-threatening injuries.
Physical examination of the pelvis should include assessment of pelvic symmetry, of the patient’s ability to stand, of sacroiliac instability, and of pain on direct palpation. A rectal examination should be performed to assess for rectal perforation or pelvic canal narrowing. The hindlimbs should be evaluated for concurrent fractures, and the stifle and tarsus assessed for palpable instability. This is especially true for any animal that is non-ambulatory.
A complete neurologic examination is indicated, as peripheral nerve and nerve root injuries are common with pelvic fractures. Fortunately, most neurologic deficits seen with pelvic fractures are transient. However loss of perineal sensation, anal tone, or hindlimb deep pain sensation are cause for cause for concern over recovery.
Anatomy and Fracture Appearance
In conjunction with the sacrum, the pelvis forms a ‘box-like’ structure. It consists of the paired bones of the ilium, acetabulum, ischium, and pubis. Single pelvic fractures are rare; damage and displacement at one point of this structure usually requires displacement at a second point.
Treatment Planning
The decision to treat pelvic fractures surgically or medically is based on a combination of computed tomography / radiographic evaluation, physical examination findings, and client/patient factors. Because it is surrounded by a significant muscle mass, the pelvis is a good biological environment for fracture healing. In many cases surgery is indicated to maximize functional outcome, relieve discomfort, and accelerate return to activity.
Surgical Management
Ilial body fractures most often appear as oblique fractures, with the fracture line extending from cranioventral to caudodorsal. The ischium commonly is displaced medially, narrowing the pelvic canal. The ilium is approached laterally, by elevation of the gluteal muscles from ventral to dorsal. Reduction is achieved by a combination of traction, levering, and use of bone holding forceps. Most ilial fractures are stabilized by plate fixation, however usage of the screws is quite common as well, however, in practice the large muscle mass and relatively narrow target for implant placement makes these techniques difficult.
A 3.5 year old Domestic Shorthair feline was referred to Northwest Referrals to undertake CT scan of the pelvis after a road traffic accident after primarily stabilisation with pain relief and additional testing for concurrent injuries.
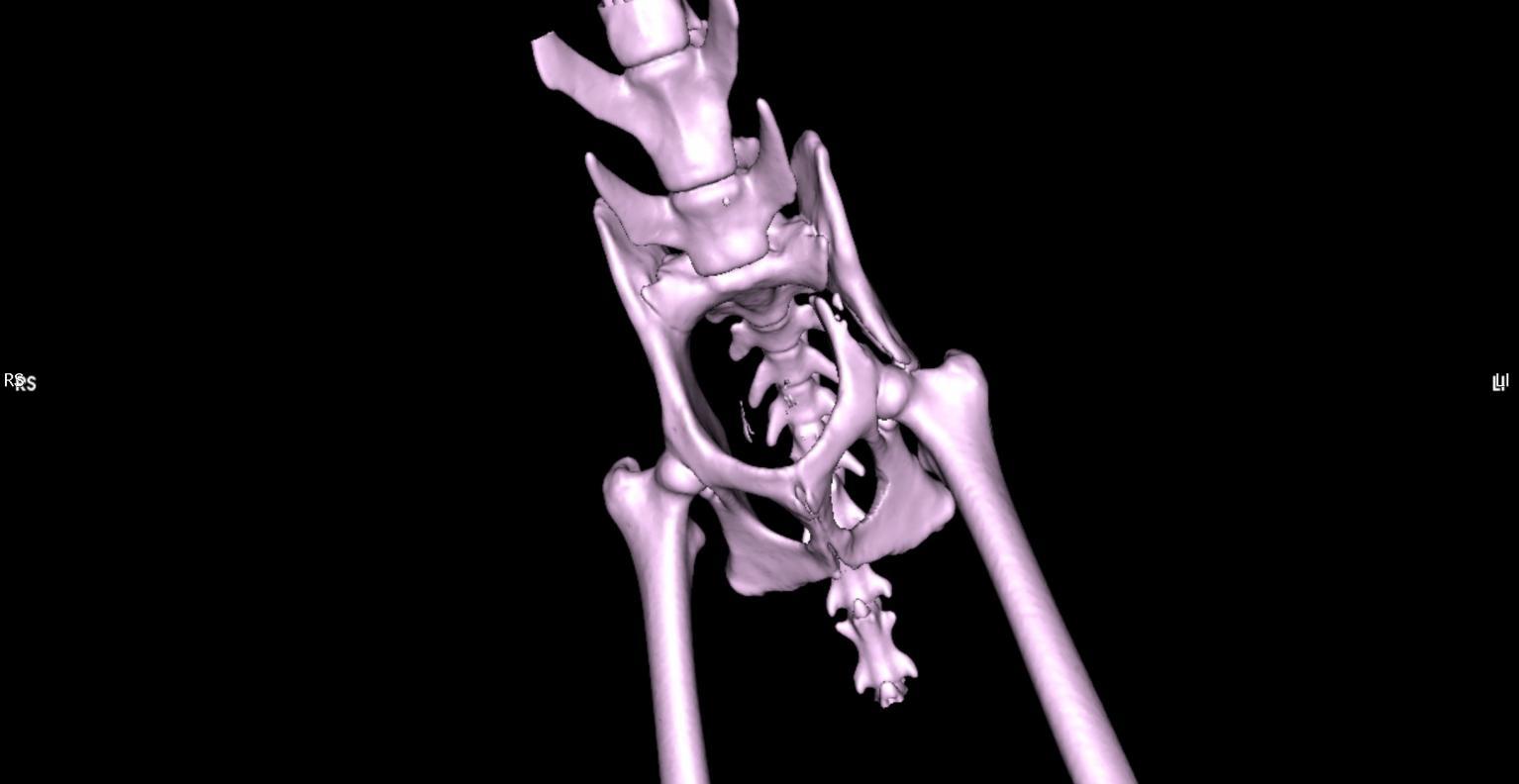
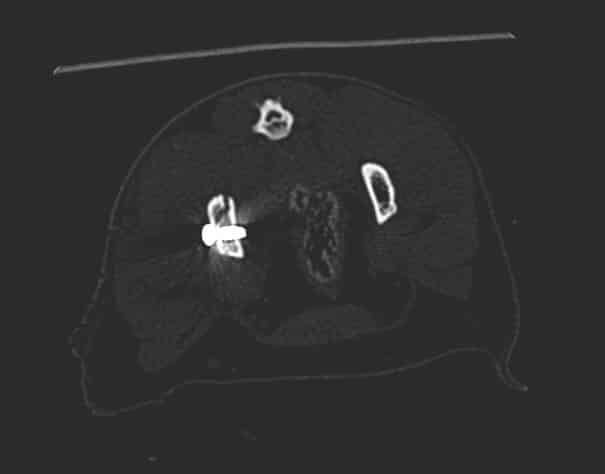
A CT scan was performed to asess the fracture and condition of the pelvis which faciliated planning of the surgery in this patient. 2 screws were placed to stabilise the fracture and he recovered well. Post CT reconstruction showed proper implant placement and fracture reduction, This gives an opportunity for the surgeon to plan the surgery itself, operate quickly and evaluate the outcome of the operation.
Fractured Pelvis
Coco – 2 year old female domestic short hair feline was referred to the Northwest Referrals with a history of a trauma followed by a road traffic accident. After primary stabilisation x-rays and CT scan of the spine limbs and pelvis were performed. Left ilium fracture was noted (fig 3.1; 3.3) and 2 cortical screws were placed to stabilise the fracture. Post op CT reconstruction was done and revealed proper positioning of the implants. (Fig 3.2; 3.4). Coco did uneventful recovery and is happy to run around in the garden chasing birds.





- difficulty rising from a sit
- trouble jumping into the car
- decreased activity level
- lameness (limping) of variable severity
- muscle atrophy (decreased muscle mass in the affected leg)
- decreased range of motion of the knee joint
- a popping noise (which may indicate a meniscal tear)
- swelling on the inside of the shin bone (fibrosis or scar tissue)
- pain
- unwillingness to play
- stiffness